Review and Javascript by Mark A. Curran, M.D. F.A.C.O.G
You can use the calculator below to calculate the doubling time of two beta hCG samples by entering the date of the blood test and the corresponding beta hCG value for that day. If the hCG level is
decreasing the the half life will be calculated.
To calculate the doubling time of two beta hCG samples:
1. Enter the date the first blood test was drawn and the beta HCG value for
the date the sample was drawn
2. Enter the date the second blood test was drawn and
the beta HCG value for the date the sample was drawn.
Ultrasonography is the preferred method to verify the presence of a viable
intrauterine gestation. [1] A gestational sac is usually seen at 5 weeks, yolk
sac at 5 1∕2 weeks, and an embryo with heartbeat at 6 weeks using transvaginal ultrasound.
The Society of Radiologists in Ultrasound Multispecialty Panel advises findings diagnostic of a pregnancy failure on
transvaginal ultrasound examination include
[2]
"
A crown-rump length 7mm or greater with no heartbeat
Mean sac diameter 25 mm or greater with no embryo
Absence of an embryo with heart beat 2 weeks or more after a scan
that showed a gestational sac without a yolk sac
Absence of embryo with heart beat 11 days or more after a scan that showed a gestational sac with a yolk sac
"
The National Institute for Health and Clinical Excellence recommends " If pregnancy failure is suspected seek a second opinion on the viability of the pregnancy and/or perform a second scan a minimum of 7 days after the first ultrasound
examination before making a diagnosis." [3]
If a woman has a positive urine or serum pregnancy
test and no intrauterine or ectopic pregnancy is seen on transvaginal
ultrasound she is considered to have a pregnancy of unknown location
which may be an early viable intrauterine pregnancy, nonviable
intrauterine pregnancy, or ectopic pregnancy .The hCG value above which
an intrauterine gestational sac would first be expected to be seen on
ultrasonography in a normal pregnancy is
called the discriminatory hCG level [2].
In the presence of an empty uterus
the likelihood of a viable pregnancy decreases
as the hCG level increases . For example, it is estimated that at
hCG levels of 2000 to 3000 mIU per milliliter, 2% of pregancies will be
viable , 65% will be nonviable , and 33% will be ectopic. At an hCG
level of more than 3000 mIU per milliliter, 0.5% of
pregancies will be viable , 66.3% nonviable, and 33.2% ectopic
[2].
Nonetheless, a live singleton birth can still result even with hCG levels above 4000 mIU/mL
and no ultrasound findings on initial examination. The discrimantory hCG level
has great variability due to hCG assay techniques , quality of ultrasound, and operator experience.
In addition, multiple gestations will have hCG levels considerably
higher than singleton gestation before ultrasound findings become
visible. Although various hCG discriminatory levels have been used to assess the risk of ectopic pregnancy, there is no established hCG level that is
diagnostic of an ectopic pregnancy [2, 4, 5].
Measurements of serum beta hCG every 48 hours may be
used to help determine viability of early intrauterine pregnancies and
to help management in pregnancies of unknown location in
hemodynamically stable patients [5] "The expected rate of increase is 49% for an initial
hCG level of less than 1,500 mIU/mL, 40% for an initial hCG level of
1,500–3,000 mIU/mL, and 33% for an initial hCG level greater than
3,000 mIU/mL" [6].
Morse and coworkers (2012) at University of
Pennsylvania School of Medicine recommend that the beta hCG level for a
successful intrauterine pregnancy should be expected to increase by at
least 35% in two days. A slower rate of increase suggests a possible
miscarriage or ectopic pregnancy. For women who are having a miscarriage
the beta hCG should be expected to fall 36 - 47% over two days. A fall
that is slower than this is suggestive of an ectopic pregnancy. About
21% of ectopic pregnancies (pregnancies implanted outside of the uterus)
have a rise in hCG similar to an intrauterine pregnancy and 8% of
ectopic pregnancies have a fall in hCG similar to a miscarriage.
Morse and coworkers conclude serial hCG values should be used in combination with clinical judgment, evaluation of symptoms and repeat ultrasound as needed.
[7]
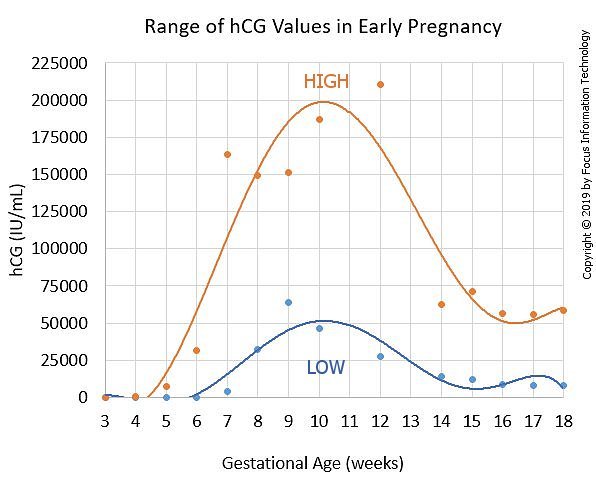
Reference Ranges for beta hCG (using
the Roche Cobas® analyzer) during the first half of pregnancy are shown below/font>
1.
Early pregnancy loss.
ACOG Practice Bulletin No. 200. American College of Obstetricians and Gynecologists. Obstet Gynecol 2018;132:e197–207.
2. Doubilet PM, Benson CB, Bourne T, Blaivas M, Barnhart KT, Benacerraf BR, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. Society of Radiologists in Ultrasound Multispecialty Panel on Early First Trimester Diagnosis of Miscarriage and Exclusion of a Viable Intrauterine Pregnancy. N Engl J Med 2013;369:1443–51.
3. National Institute for Health and Clinical Excellence. Ectopic pregnancy
and miscarriage: diagnosis and initial management in early pregnancy of
ectopic pregnancy and miscarriage. NICE Clinical Guideline 126.
Manchester (UK): NICE; 2012. Available
at:https://www.nice.org.uk/guidance/ng126/resources/ectopic-pregnancy-and-miscarriage-diagnosis-and-initial-management-pdf-66141662244037.
Retrieved July 25, 2019. (Level III) 4.Doubilet PM, Benson
CB.Further evidence against the reliability of the human chorionic
gonadotropin discriminatory level. J Ultrasound Med. 2011
Dec;30(12):1637-42. PMID: 22123998 5. Tubal ectopic pregnancy.
ACOG Practice Bulletin No. 193. American College of Obstetricians and
Gynecologists. Obstet Gynecol 2018;131:e91–103. 6.
Barnhart KT, et al. Differences in Serum Human Chorionic Gonadotropin
Rise in Early Pregnancy by Race and Value at Presentation. Obstet
Gynecol. 2016 Sep;128(3):504-11.PMID: 27500326 7.
.Morse CB, et. Al., Performance of human chorionic gonadotropin curves in women at risk for ectopic pregnancy: exceptions to the rules. Fertil Steril. 2012 Jan;97(1):101-6.e2.
PMID:22192138 8. Human Chorionic Gonadotropin (hCG) on Elecsys 1010/2010 and Modular Analytics
E170 [package insert 2007-2009, VII] Indianapolis,Ind;Roche
All calculations must be confirmed before use. The suggested results are not a substitute for clinical
judgment. Neither perinatology.com nor any other party involved in the preparation or publication of this site shall be liable for any special, consequential,
or exemplary damages resulting in whole or part from any user's use of or reliance upon this material.